COVID-19 Superspreader Events in 28 Countries: Critical Patterns and Lessons
In the absence of any comprehensive database of COVID-19 superspreading events, I built my own.
Jonathan Kay
· 21 min read
A collection of 14 posts
In the absence of any comprehensive database of COVID-19 superspreading events, I built my own.

Talat Chughtai, Director of the Trauma Intensive Care Unit at Hamad General Hospital, talks to Jonathan Kay about COVID-19, the strain it’s putting on health-care systems, and what we’ve learned from China about how best to treat it.
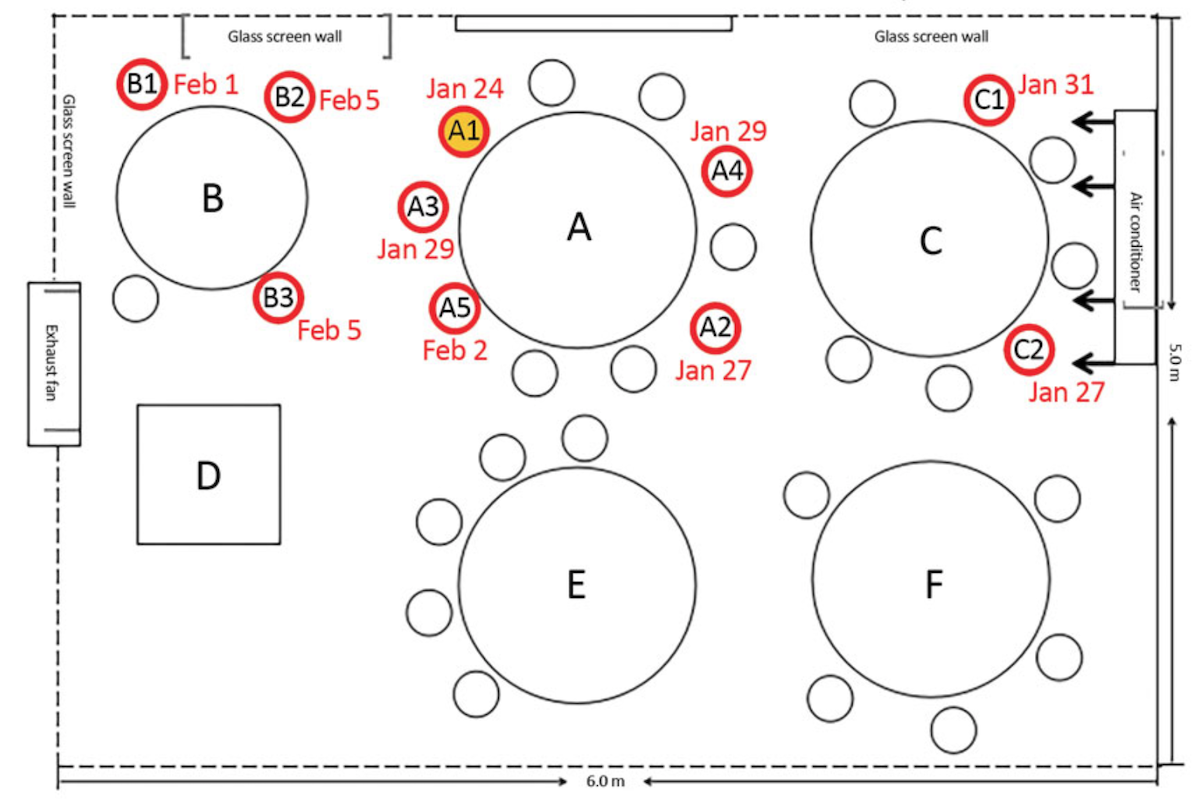
Both the scientific literature and media reports suggest COVID-19 transmission is most likely to take place (1) within families, and (2) through one-off SSEs of the type described above.
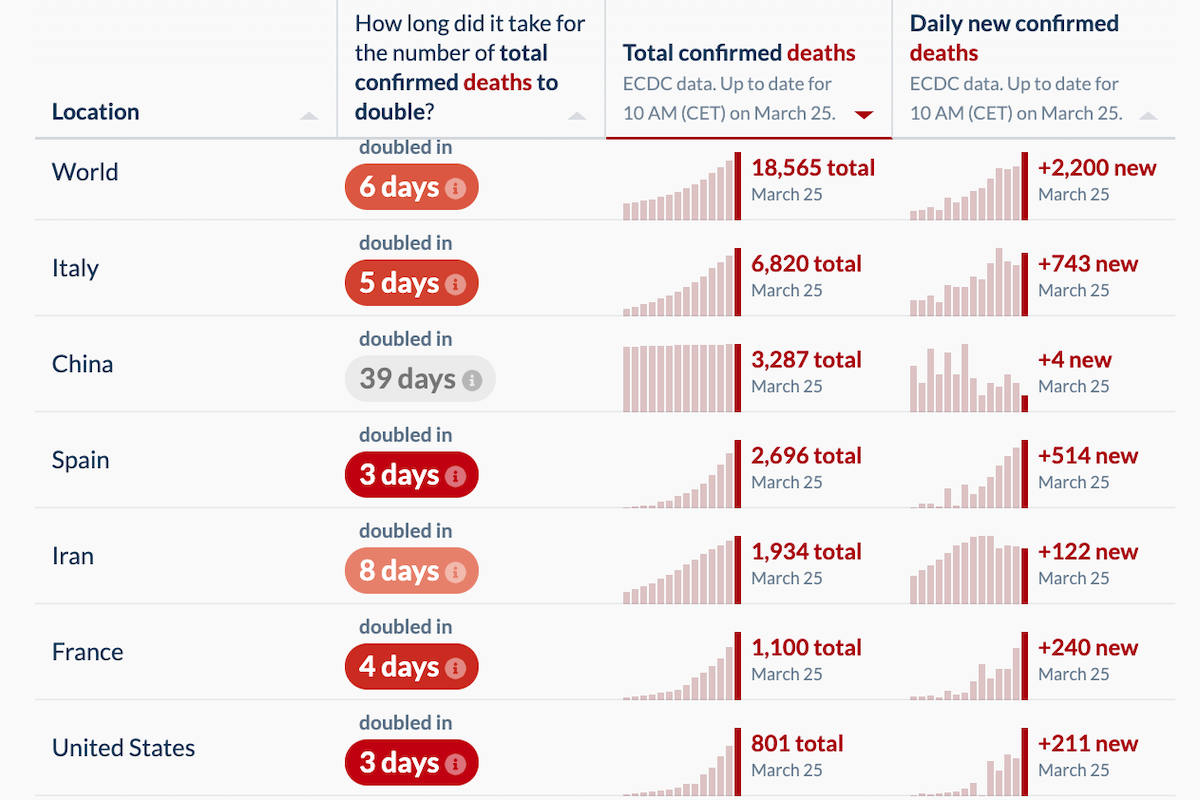
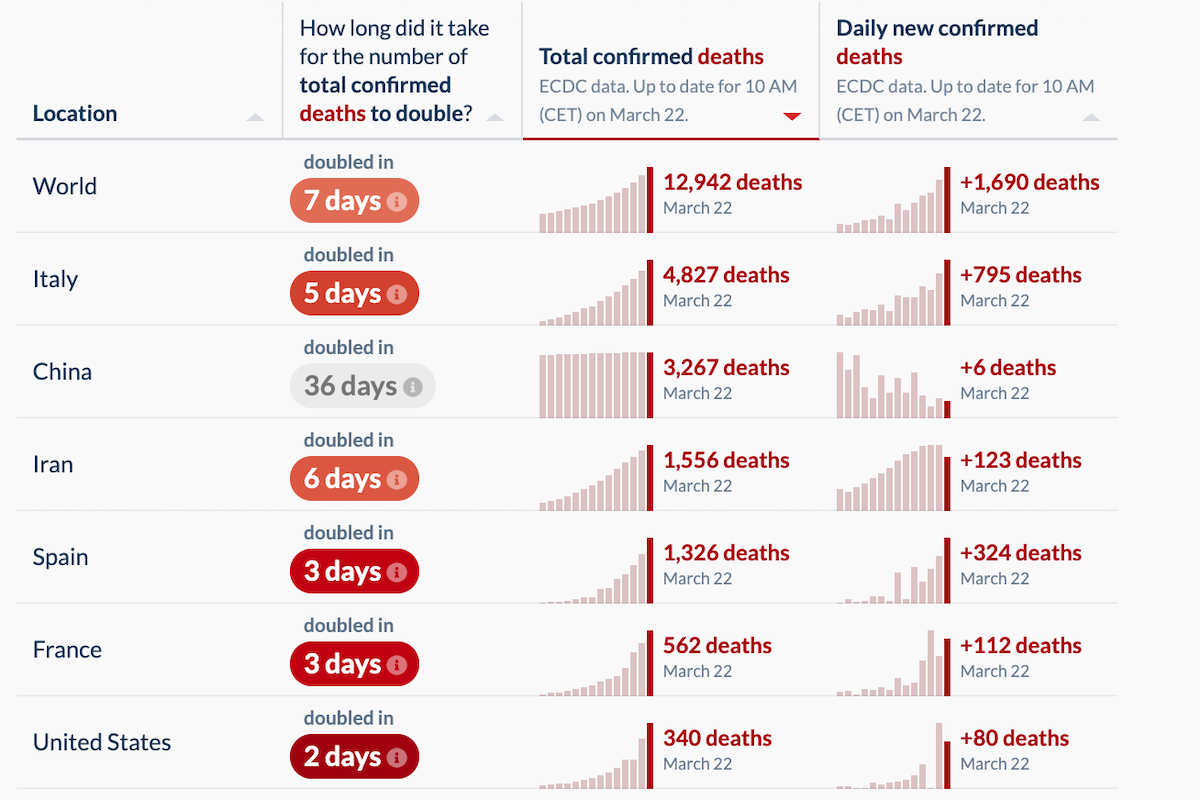
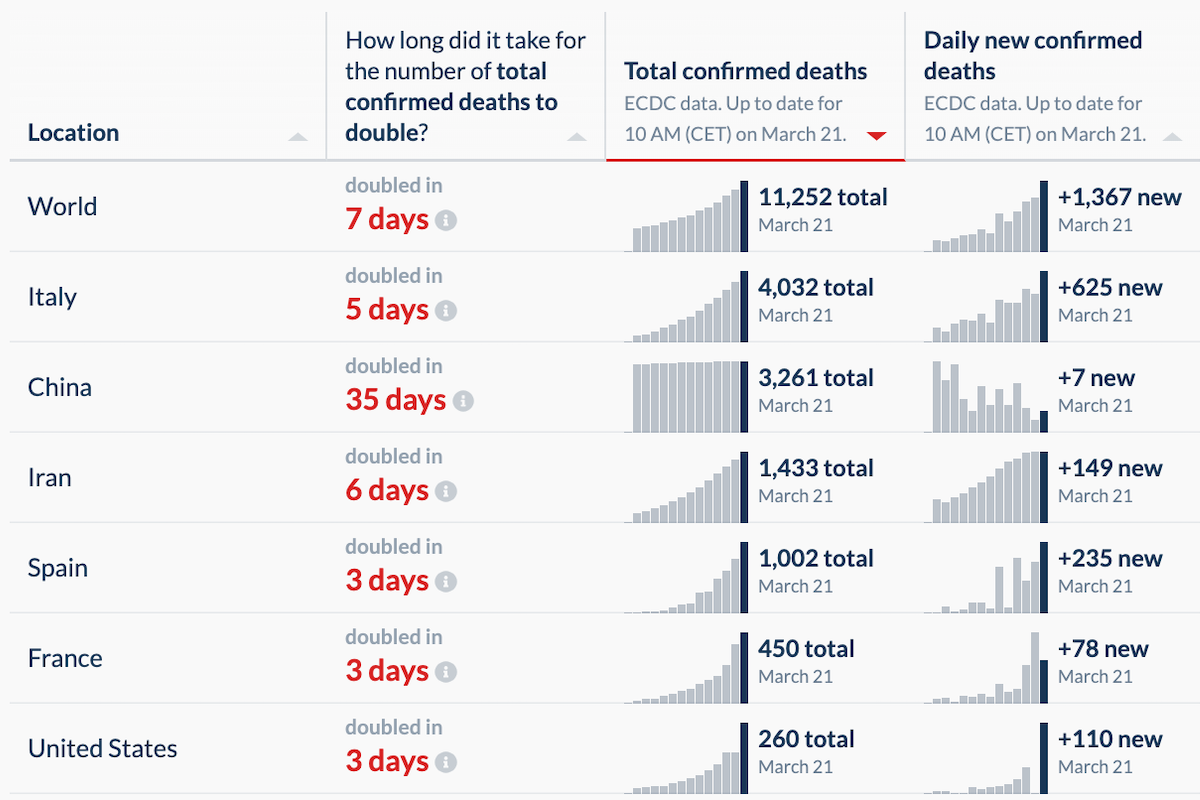
According to statistics compiled by Our World in Data (OWD), the number of newly confirmed COVID-19 deaths decreased yesterday.
The latest research on COVID-19 tells us that “the major transmission mechanisms are not fine aerosols but large droplets.”
On an annualized basis, the last three weeks in Lombardy correspond to a regional per-capita death rate of 0.72 percent—or, put another way, the death of one person out of every 140 residents.
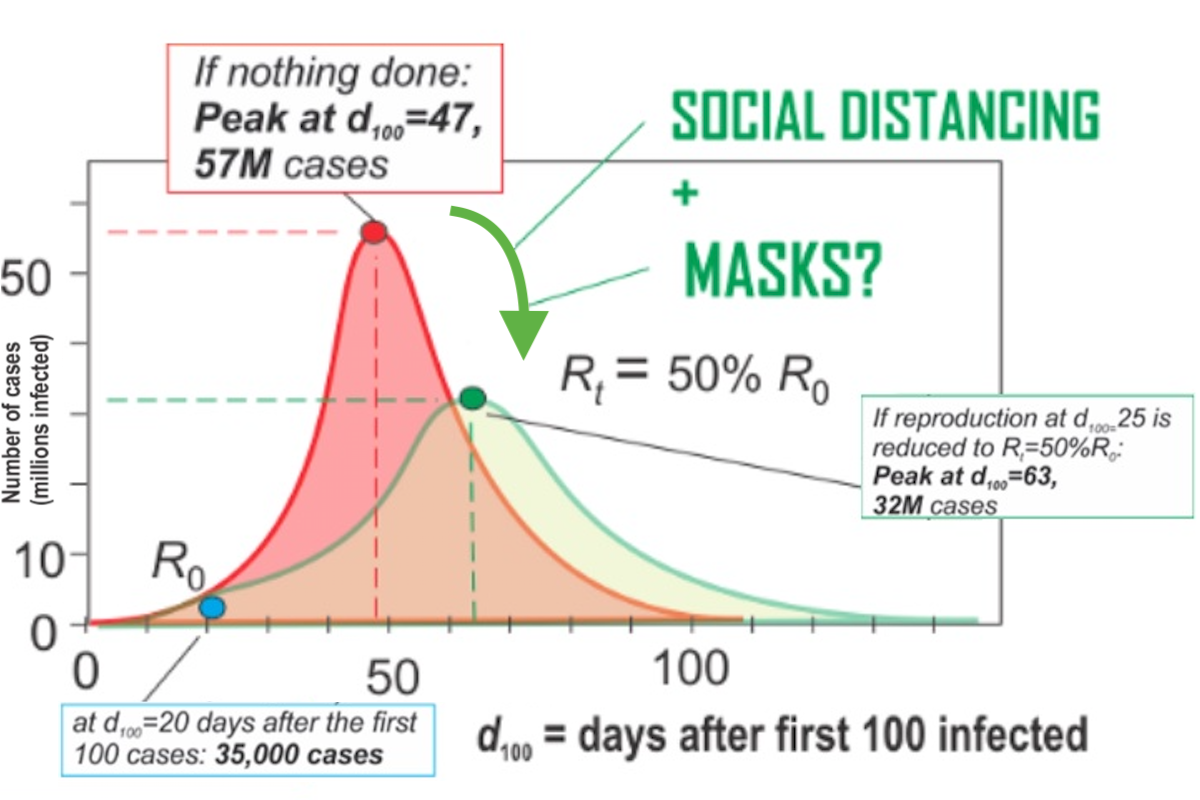
Absent isolation or other precautionary measures, the average socially active COVID-19 infectee will transmit the disease to an average of about 2.4 people. i.e., the R0 value is 2.4. But super-spreaders can spread a disease to dozens or hundreds.
Even if a COVID-19 vaccine were invented tomorrow (it won’t be), our experience with the virus shows how underprepared we are for this kind of public-health emergency.
This clustering phenomenon explains why the COVID-19 policy debate among politicians, doctors, and pundits now has become somewhat surreal, with world-class experts telling us either that we are facing an “apocalypse,” or that the pandemic will fizzle and we’re all “going to be fine.”

The analysis here is complicated, because a massive testing regime doesn’t seem to be a necessary component of COVID-19 suppression.

For the first time in a week, the daily number of new global confirmed COVID-19 deaths has dropped—from 1,690 to 1,660. That’s a small drop, but it’s important.
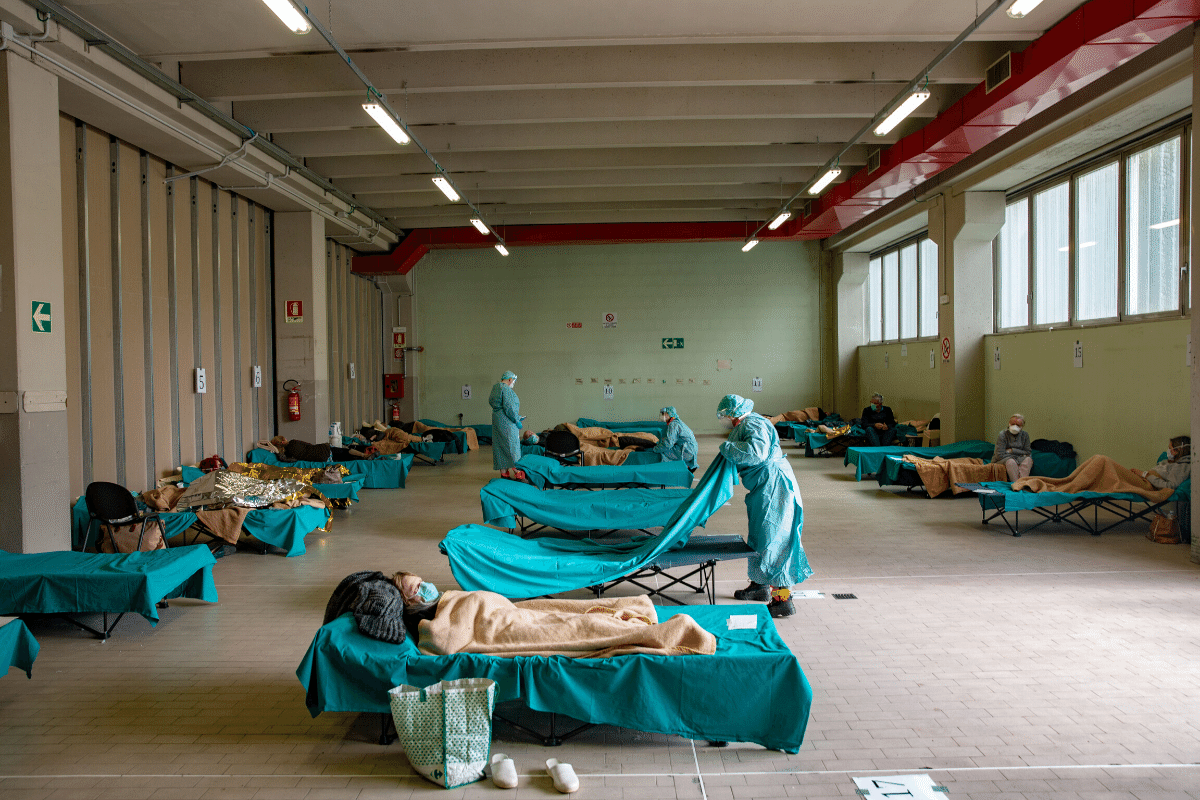
The problem isn’t just the number of ventilators and ICU beds, but also the limited number of staff who can operate such equipment.
There are reports of ventilator shortages, and the possibility of an Italian-style horror show, with doctors deciding whose parents live and whose parents die, seems real.
The World Health Organization announced last week that Europe is now the epicentre of the new coronavirus epidemic. As the announcement was made, many countries in Africa and Asia were imposing strict restrictions on the arrival of flights and visitors from Europe. It felt like a great historical reversal, one